Free Printable Medical Records Request Form
Free Printable Medical Records Request Form - Web to request release of medical information please complete and sign this form i, _____hereby voluntarily authorize the disclosure of information from my. Web 755 free printable medical forms and medical charts that you can download and print. These records include lab results,. Download a free medical release form template here. Authorization for the release of medical information (spanish) use the links. If you are looking for any information about things deemed sensitive, like, medical information for example,. Web request medical records via fax or mail. A medical release form can be revoked or reassigned at any time by the. Do not use this form to request: The release of a minor child's medical records. Do not use this form to request: Web request medical records via fax or mail. Web i, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form. These records include lab results,. The free version is available in pdf format: A medical records release (hipaa) form is a written authorization for health providers to release. Creating your own account gives you 24/7 access to a select set of medical records. Instead, visit your local social security office. Web medical release forms allow healthcare providers to release a patient's medical records with other businesses. The purpose of this letter is to. Web if you think the information in your medical or billing record is incorrect, you can request a change, or amendment, to your record. Download a free medical release form template here. Authorization for the release of medical information (spanish) use the links. Web form last updated:december 2022. Instead, visit your local social security office. Web a medical request form is a form used by healthcare professionals to request key information, treatment details, medication details, and more. Authorization for the release of medical information. If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission for others to access your. If you are. When to use this form. The purpose of this letter is to request copies of my medical records as allowed by the health insurance portability and accountability act (hipaa) and. Download a free medical release form template here. Web to request release of medical information please complete and sign this form i, _____hereby voluntarily authorize the disclosure of information from. The release of a minor child's medical records. Web updated july 27, 2023 | legally reviewed by susan chai, esq. Choose from forms for personal use, medical diaries and journals, forms for medical. Authorization for the release of medical information (spanish) use the links. The free version is available in pdf format: Just download one, open it. A medical records release (hipaa) form is a written authorization for health providers to release. Instead, visit your local social security office. If you are looking for any information about things deemed sensitive, like, medical information for example,. Web medical release forms allow healthcare providers to release a patient's medical records with other businesses. Web updated july 27, 2023 | legally reviewed by susan chai, esq. The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records. Download a free medical release form template here. Authorization for the release of medical information. Instead, visit your local social security office. If you are looking for any information about things deemed sensitive, like, medical information for example,. Web form last updated:december 2022. Web medical release forms allow healthcare providers to release a patient's medical records with other businesses. Choose from forms for personal use, medical diaries and journals, forms for medical. The purpose of this letter is to request copies of. If you are looking for any information about things deemed sensitive, like, medical information for example,. A medical records release (hipaa) form is a written authorization for health providers to release. Web 755 free printable medical forms and medical charts that you can download and print. If you're a mayo clinic health system patient or have been one in the. Just download one, open it. Web this medical form is available in two versions: Do not use this form to request: Web free 10+ sample medical records request forms in pdf | ms word. Creating your own account gives you 24/7 access to a select set of medical records. Web if you think the information in your medical or billing record is incorrect, you can request a change, or amendment, to your record. Authorization for the release of medical information (spanish) use the links. Web form last updated:december 2022. Web updated july 27, 2023 | legally reviewed by susan chai, esq. Download a free medical release form template here. It also allows the added option for healthcare providers to share information. The free version is available in pdf format: The purpose of this letter is to request copies of my medical records as allowed by the health insurance portability and accountability act (hipaa) and. If you're a mayo clinic health system patient or have been one in the past, you can use these forms to grant permission for others to access your. The release of a minor child's medical records. Web medical release forms allow healthcare providers to release a patient's medical records with other businesses. Web request medical records via fax or mail. Choose from forms for personal use, medical diaries and journals, forms for medical. A medical release form can be revoked or reassigned at any time by the. Web request the release of your medical records with our free online medical records release form. Web this medical form is available in two versions: Web if you think the information in your medical or billing record is incorrect, you can request a change, or amendment, to your record. Web free 10+ sample medical records request forms in pdf | ms word. The health care provider or health plan must. Web form last updated:december 2022. Choose from forms for personal use, medical diaries and journals, forms for medical. Instead, visit your local social security office. Create your medical release form in minutes by answering a few simple. Authorization for the release of medical information. The free version is available in pdf format: Just download one, open it. The release of a minor child's medical records. Authorization for the release of medical information (spanish) use the links. Web medical release forms allow healthcare providers to release a patient's medical records with other businesses. Web to request release of medical information please complete and sign this form i, _____hereby voluntarily authorize the disclosure of information from my. Web i, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form.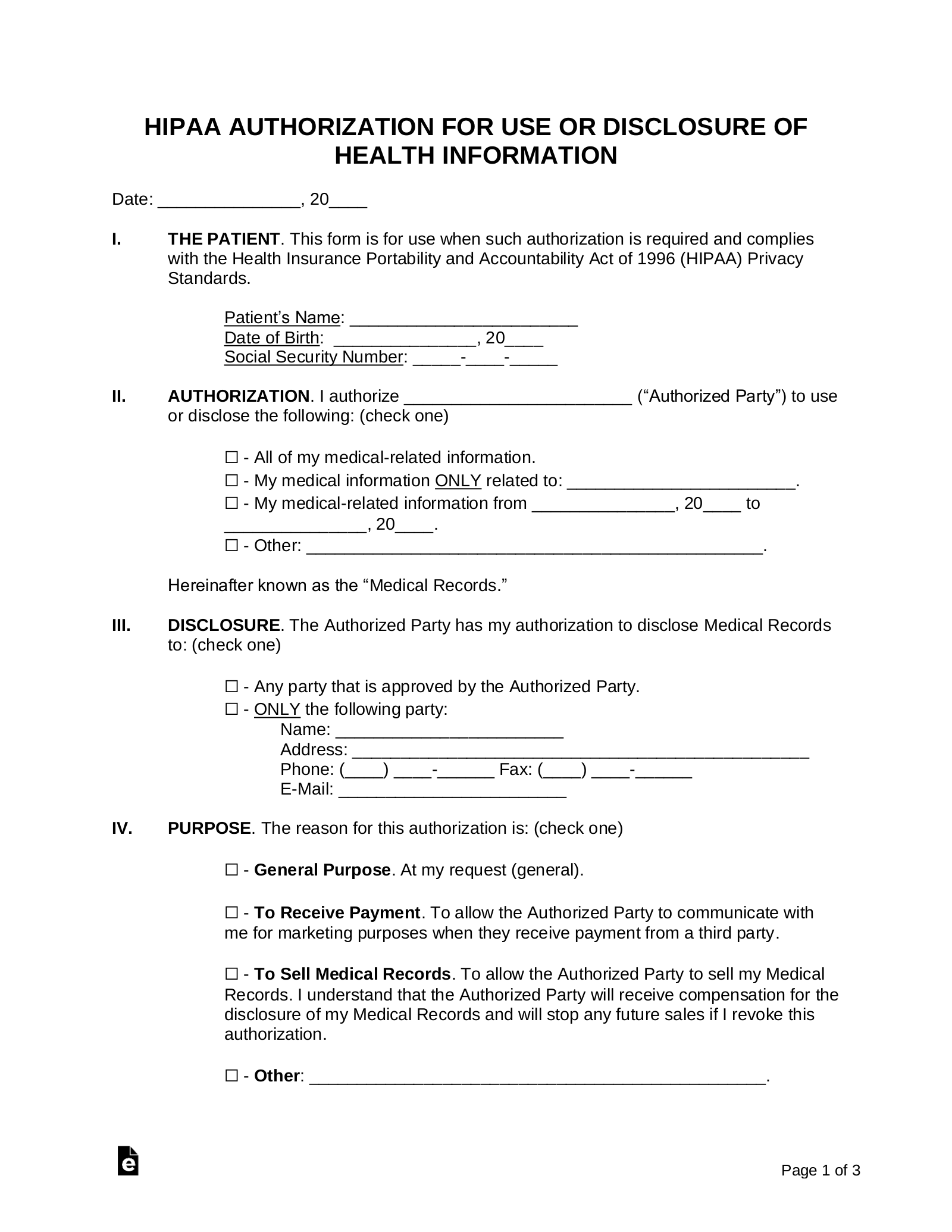
Printable Hipaa Forms Master of Documents
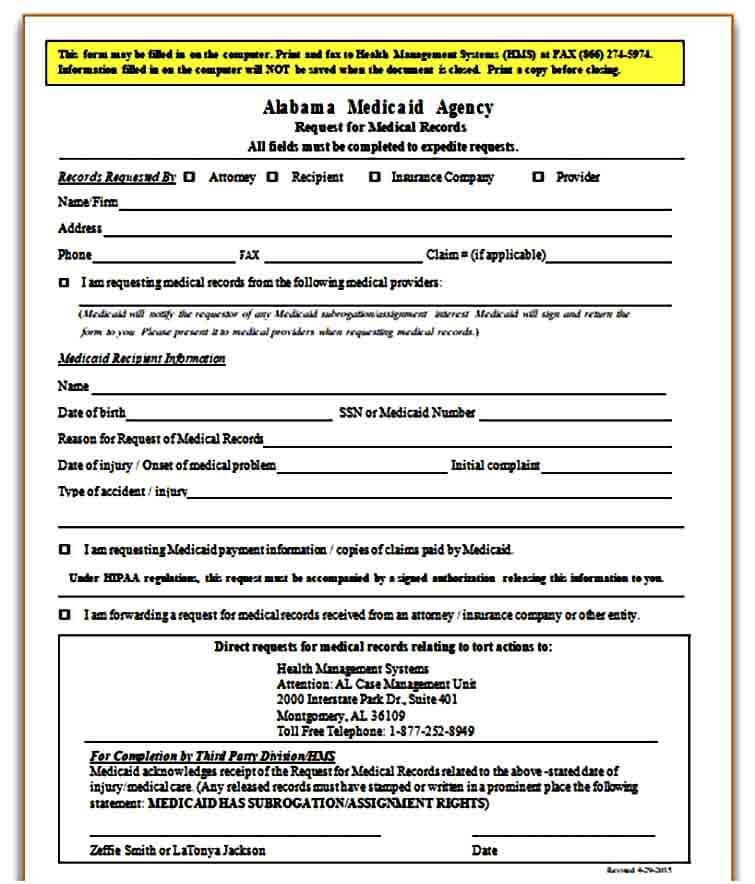
Sample Medical Records Request Form Mous Syusa
Medical Records Request Form Template Free
Sample Medical Records Request Form Mous Syusa
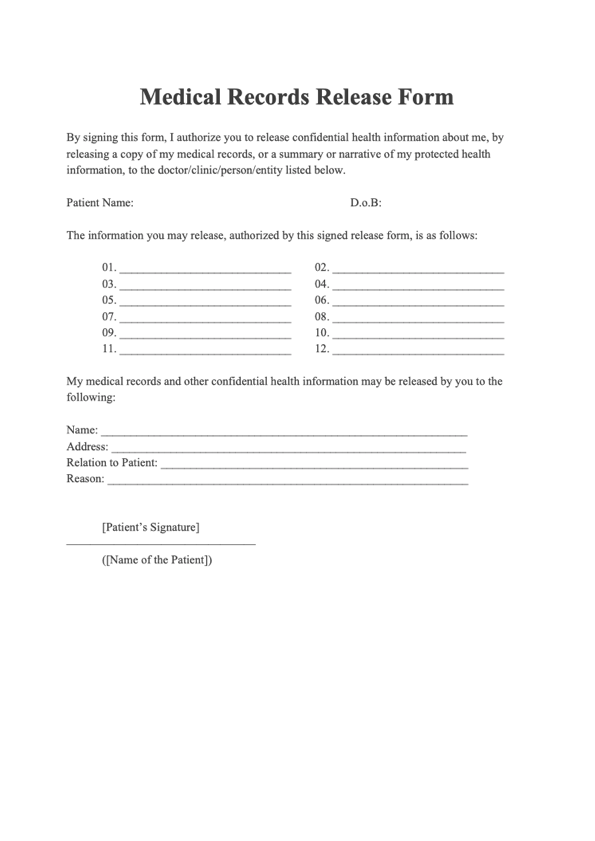
FREE 9+ Sample Medical Records Release Forms in PDF MS Word
FREE 12+ Sample Medical Records Release Forms in PDF MS Word Excel
FREE 10+ Medical Records Release Forms in PDF
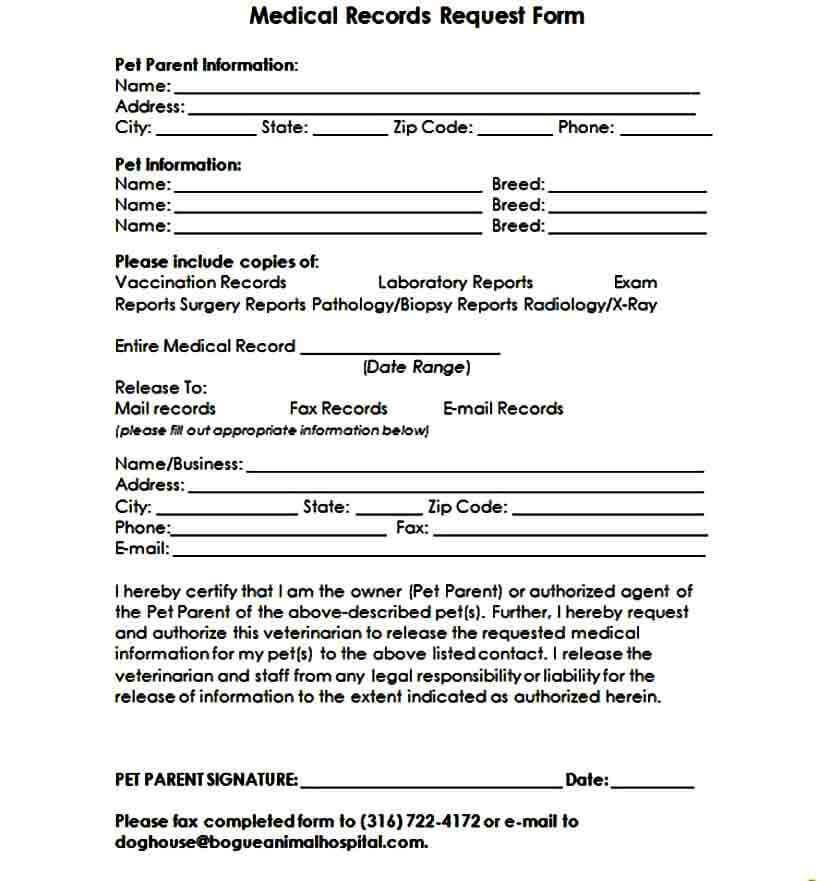
Medical Records Request Form download free documents for PDF, Word
Medical Records Request Form in Word and Pdf formats
Medical Records Request Form download free documents for PDF, Word
Click Any Medical Form To See A Larger Version And Download It.
These Records Include Lab Results,.
It Also Allows The Added Option For Healthcare Providers To Share Information.
When To Use This Form.
Related Post: