Printable Dental Clearance Form
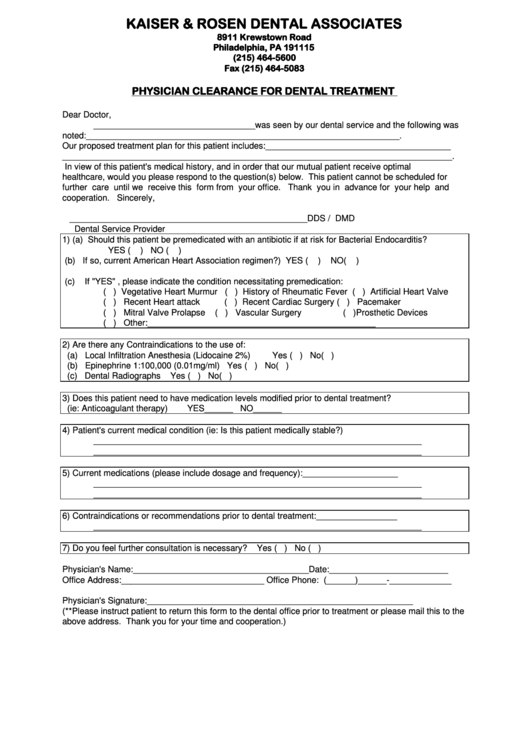
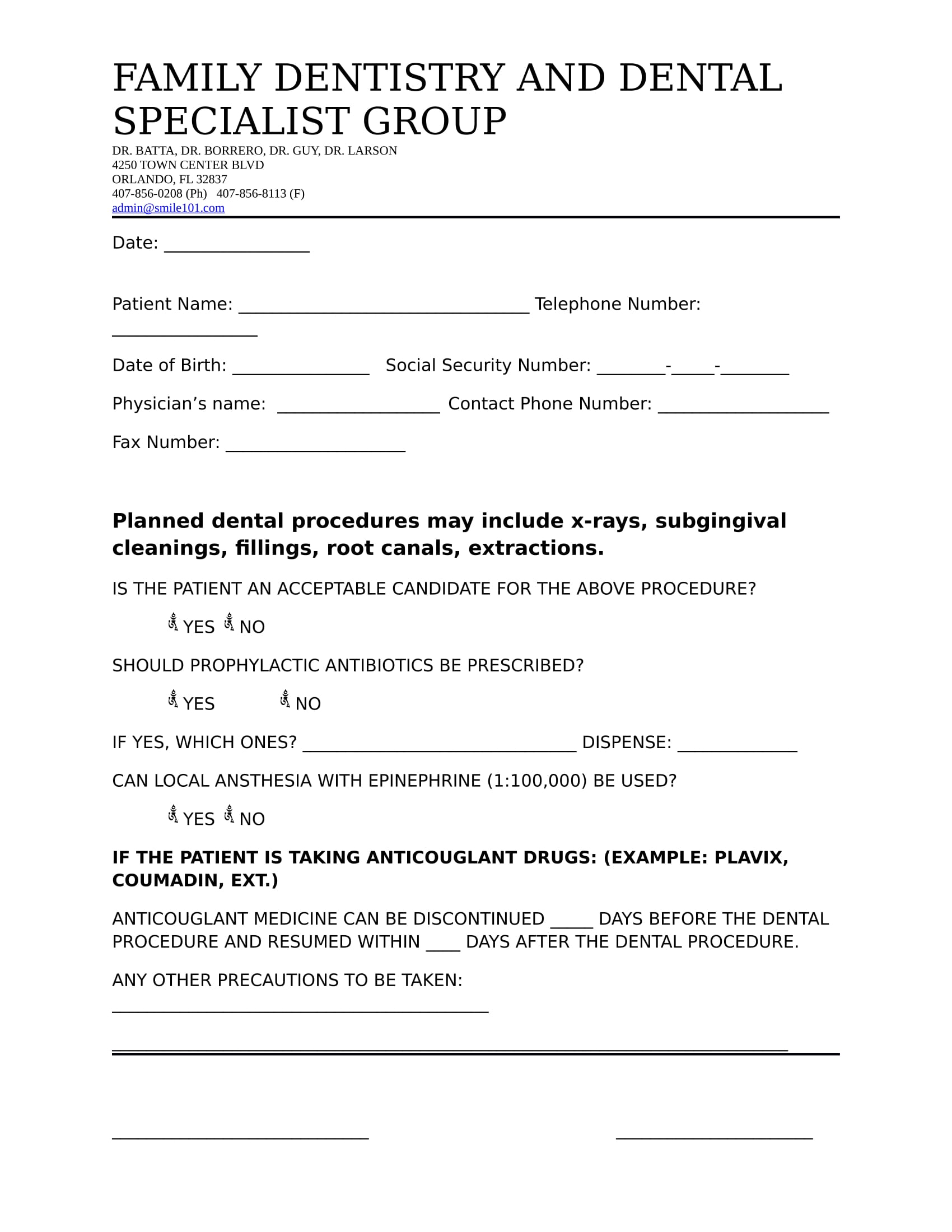
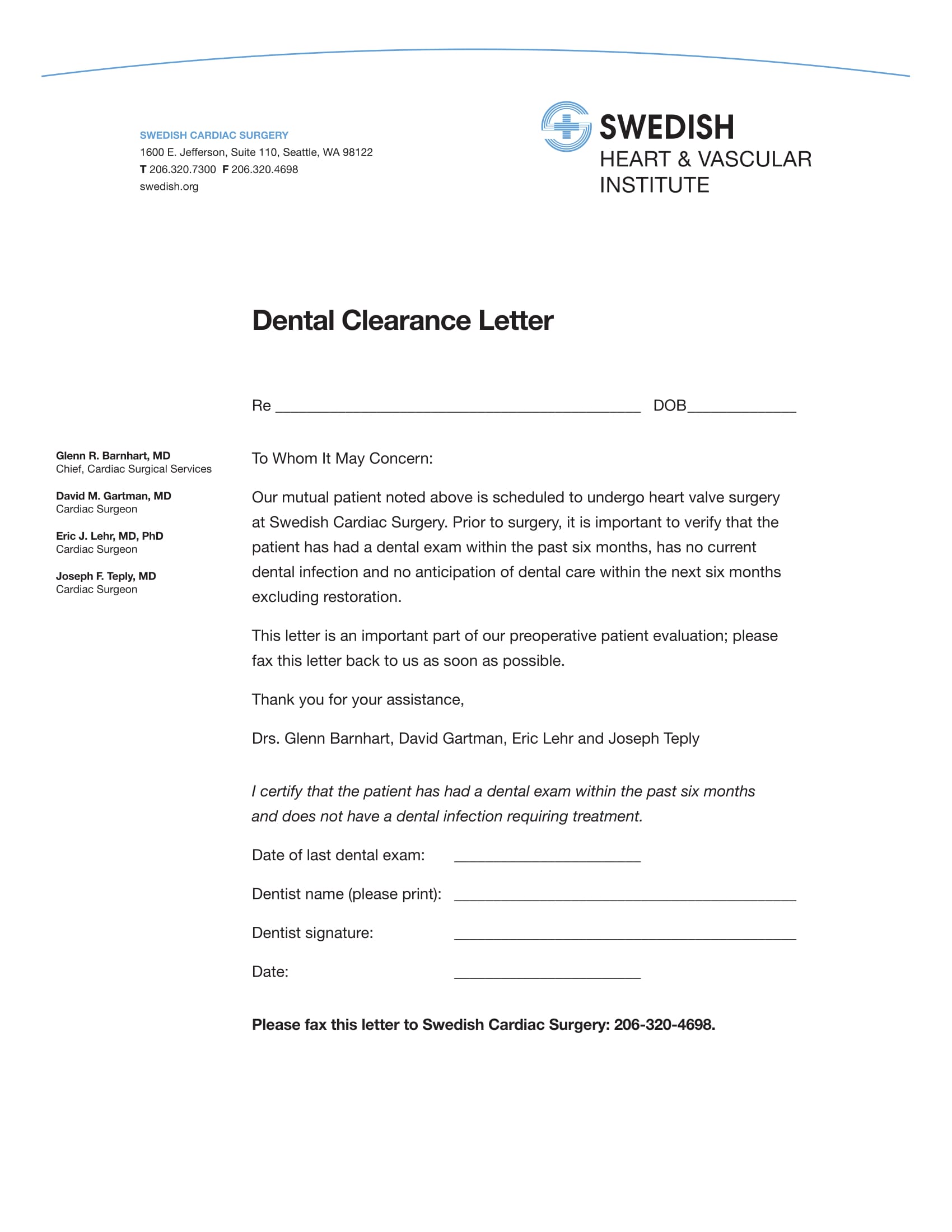
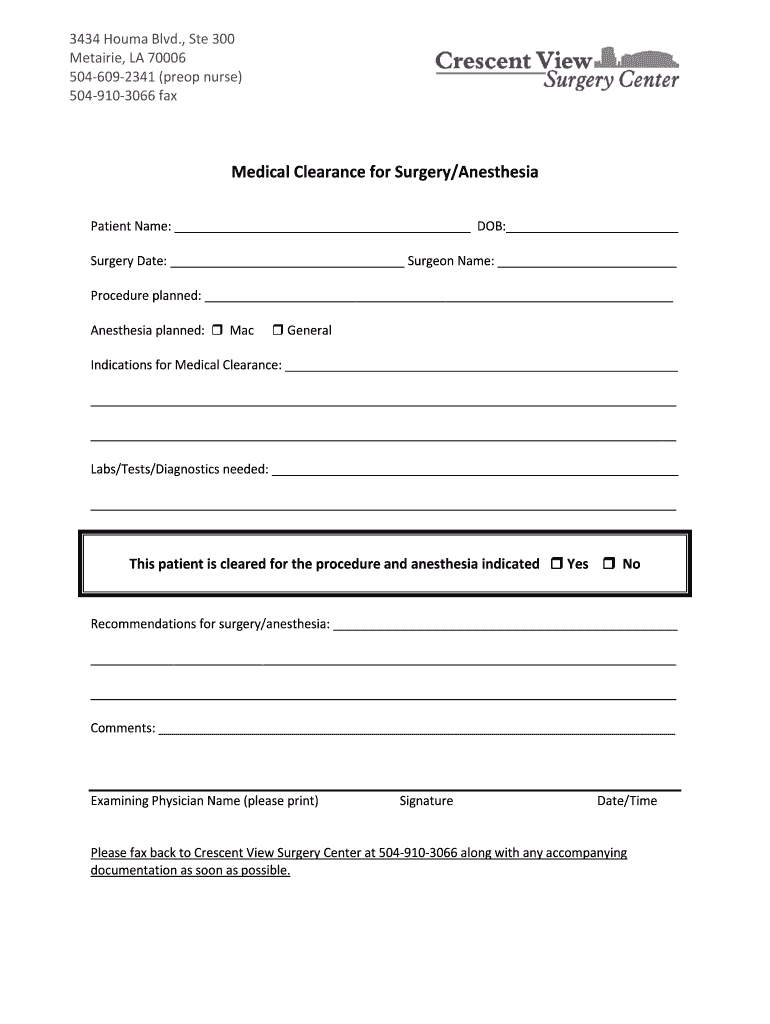
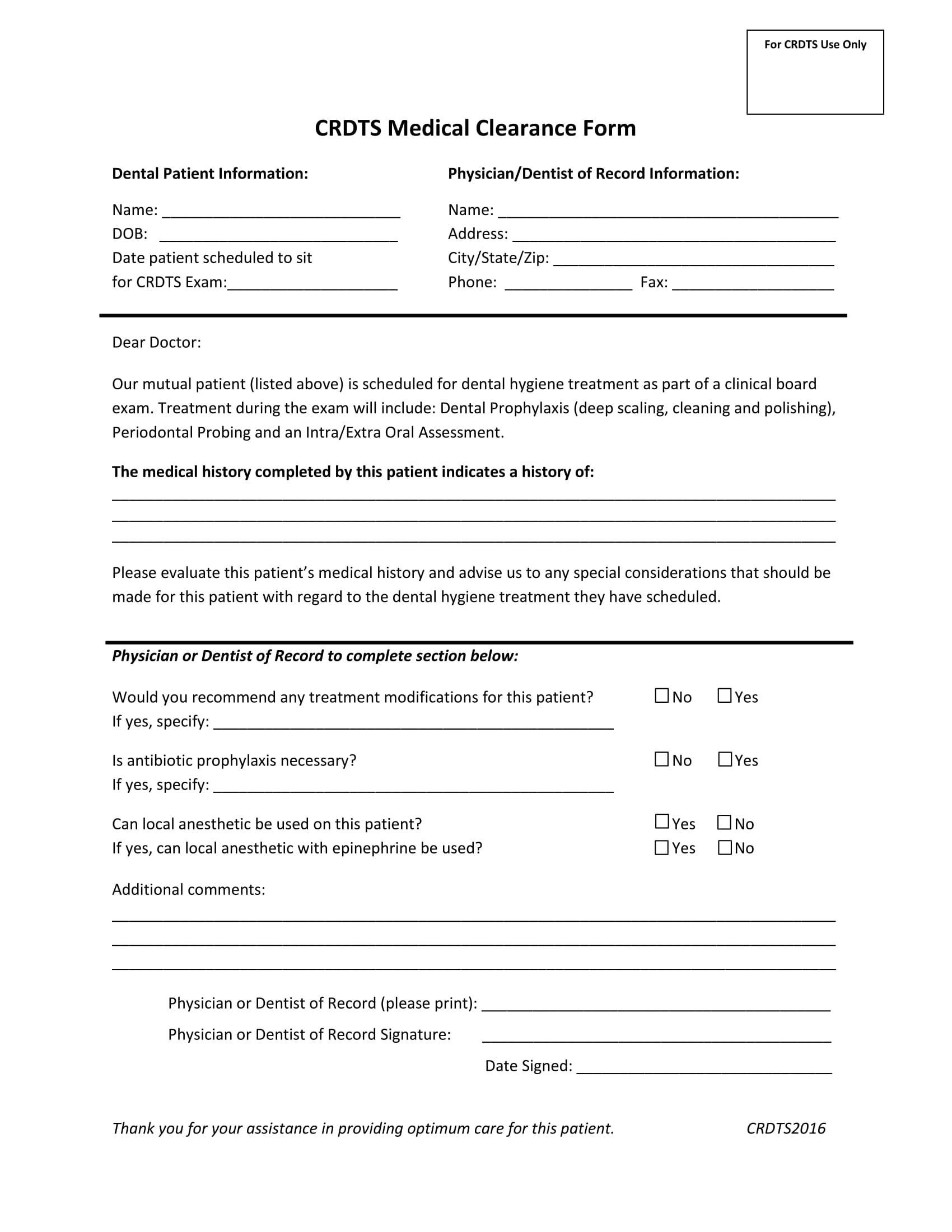
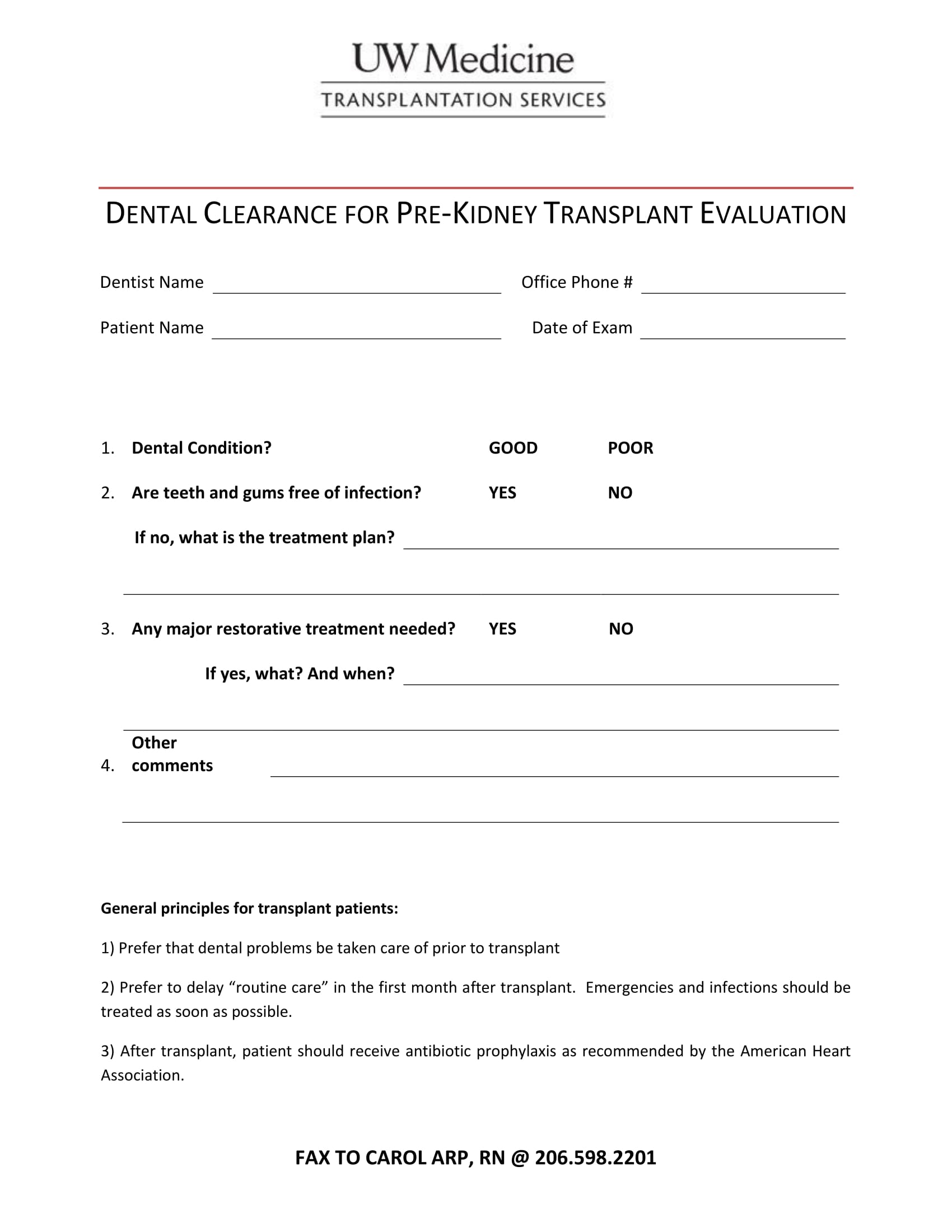
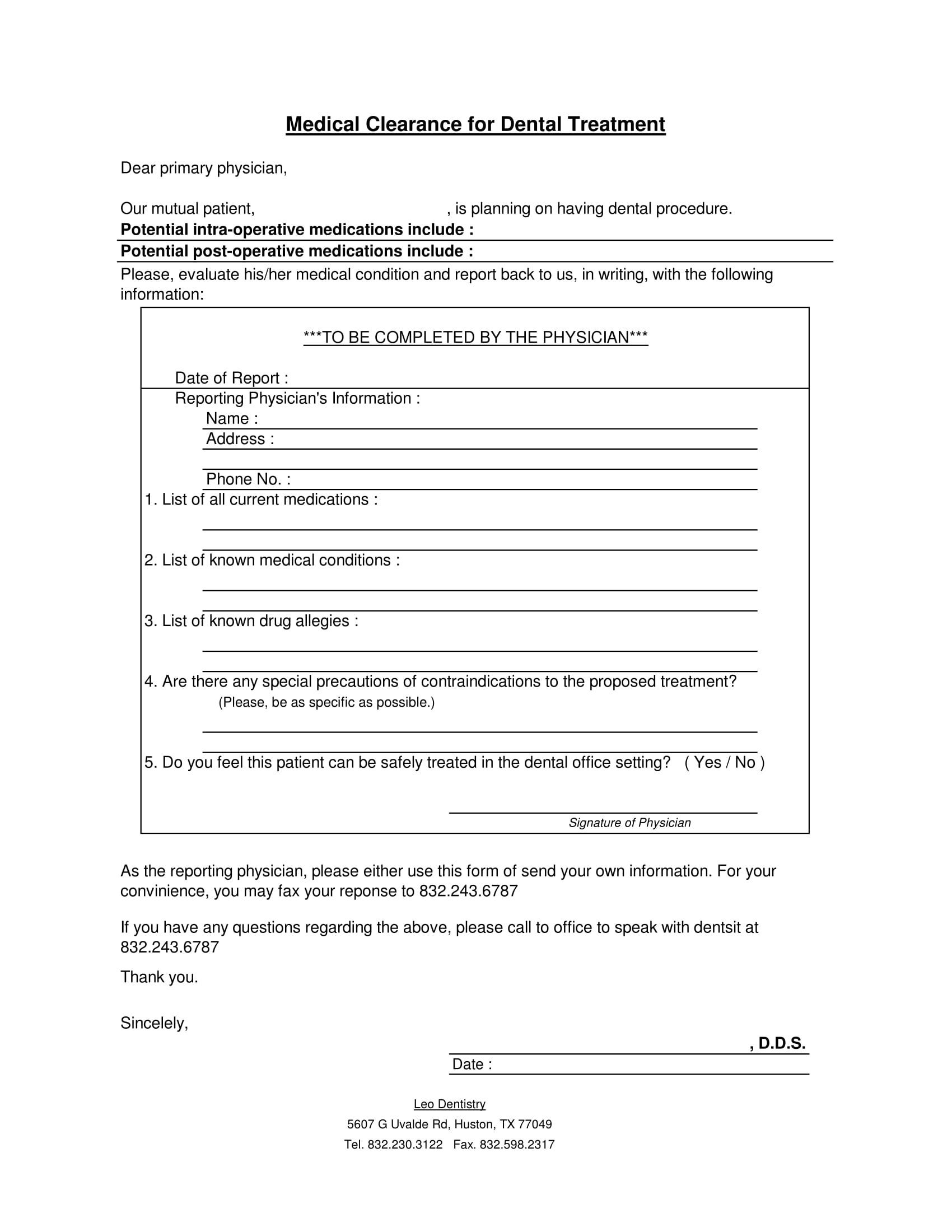
Printable Dental Clearance Form - Web dental clearance form please have your dentist complete all sections of this form and fax it to 216.445.9608 if you have had your teeth. Save or instantly send your ready documents. Easily fill out pdf blank, edit, and sign them. Web prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active cavities, gum disease,. Web complete dental clearance letter online with us legal forms. Web share your form with others. Web find the dental clearance letter you want. Easily fill out pdf blank, edit, and sign them. You can also download it, export it or print it out. Upload printable dental clearance form for surgery from your device, the cloud, or a secure link. Web click on new document and choose the form importing option: Web prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active cavities, gum disease,. Edit your dental clearance form pdf online. Web utilize the upper and left panel tools to redact. Web searching for printable dental clearance form to fill? Web medical clearance for dental treatment. Web complete medical clearance for dental surgery online with us legal forms. This patient has had a dental exam within the past 2 years this patient has had a dental cleaning within the past 6 months the patient does not have an active dental. Web. Web complete medical clearance form for dental online with us legal forms. Web complete medical clearance for dental surgery online with us legal forms. Easily fill out pdf blank, edit, and sign them. Web find the dental clearance letter you want. Web the electronic form is designed for oral health providers to enter information into specific fields in the form. Web find the dental clearance letter you want. Save or instantly send your ready documents. This patient has had a dental exam within the past 2 years this patient has had a dental cleaning within the past 6 months the patient does not have an active dental. Web dental clearance form please have your dentist complete all sections of this. Web complete medical clearance form for dental online with us legal forms. Web prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active cavities, gum disease,. Web the electronic form is designed for oral health providers to enter information into specific fields. Web click on new document and choose the form importing option: However, failure to provide the information requested. The dentist must indicate if the patient is suitable for dental. Web share your form with others. Web the electronic form is designed for oral health providers to enter information into specific fields in the form. Web share your form with others. Easily fill out pdf blank, edit, and sign them. You can edit these pdf forms online and download them on your computer for free. Web complete medical clearance for dental surgery online with us legal forms. Save or instantly send your ready documents. You can also download it, export it or print it out. However, failure to provide the information requested. This patient has had a dental exam within the past 2 years this patient has had a dental cleaning within the past 6 months the patient does not have an active dental. Web prior to surgery, it is important to verify that. Upload printable dental clearance form for surgery from your device, the cloud, or a secure link. Insert and customize text, pictures, and fillable areas, whiteout unneeded. Easily fill out pdf blank, edit, and sign them. Web the electronic form is designed for oral health providers to enter information into specific fields in the form. Save or instantly send your ready. Web dental clearance form please have your dentist complete all sections of this form and fax it to 216.445.9608 if you have had your teeth. Send dental clearance via email, link, or fax. Easily fill out pdf blank, edit, and sign them. The dentist must indicate if the patient is suitable for dental. Upload printable dental clearance form for surgery. Web share your form with others. Send dental clearance via email, link, or fax. Edit your dental clearance form pdf online. Easily fill out pdf blank, edit, and sign them. Involved parties names, addresses and phone numbers etc. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. You can also download it, export it or print it out. Easily fill out pdf blank, edit, and sign them. Web complete dental clearance letter online with us legal forms. Web click on new document and choose the form importing option: However, failure to provide the information requested. Insert and customize text, pictures, and fillable areas, whiteout unneeded. Upload printable dental clearance form for surgery from your device, the cloud, or a secure link. Web dd form 2813, nov 2021. Web prior to surgery, it is important to verify that the patient has had a dental exam within the past 6 months, has no current dental infection, no active cavities, gum disease,. Save or instantly send your ready documents. Web the dental clearance form template is a document provided by a dentist and addressed to another physician. Save or instantly send your ready documents. Save or instantly send your ready documents. Web complete medical clearance form for dental online with us legal forms. However, failure to provide the information requested. Web complete medical clearance for dental surgery online with us legal forms. You can edit these pdf forms online and download them on your computer for free. Web click on new document and choose the form importing option: Insert and customize text, pictures, and fillable areas, whiteout unneeded. Save or instantly send your ready documents. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. Web share your form with others. Web complete dental clearance letter online with us legal forms. You can also download it, export it or print it out. Web utilize the upper and left panel tools to redact printable medical clearance form for dental treatment. Web complete medical clearance form for dental online with us legal forms. Web physician name (please print): Save or instantly send your ready documents. Involved parties names, addresses and phone numbers etc. (please print)_____ physician signature:_____ date:_____ we appreciate your assistance in providing optimum care for this patient.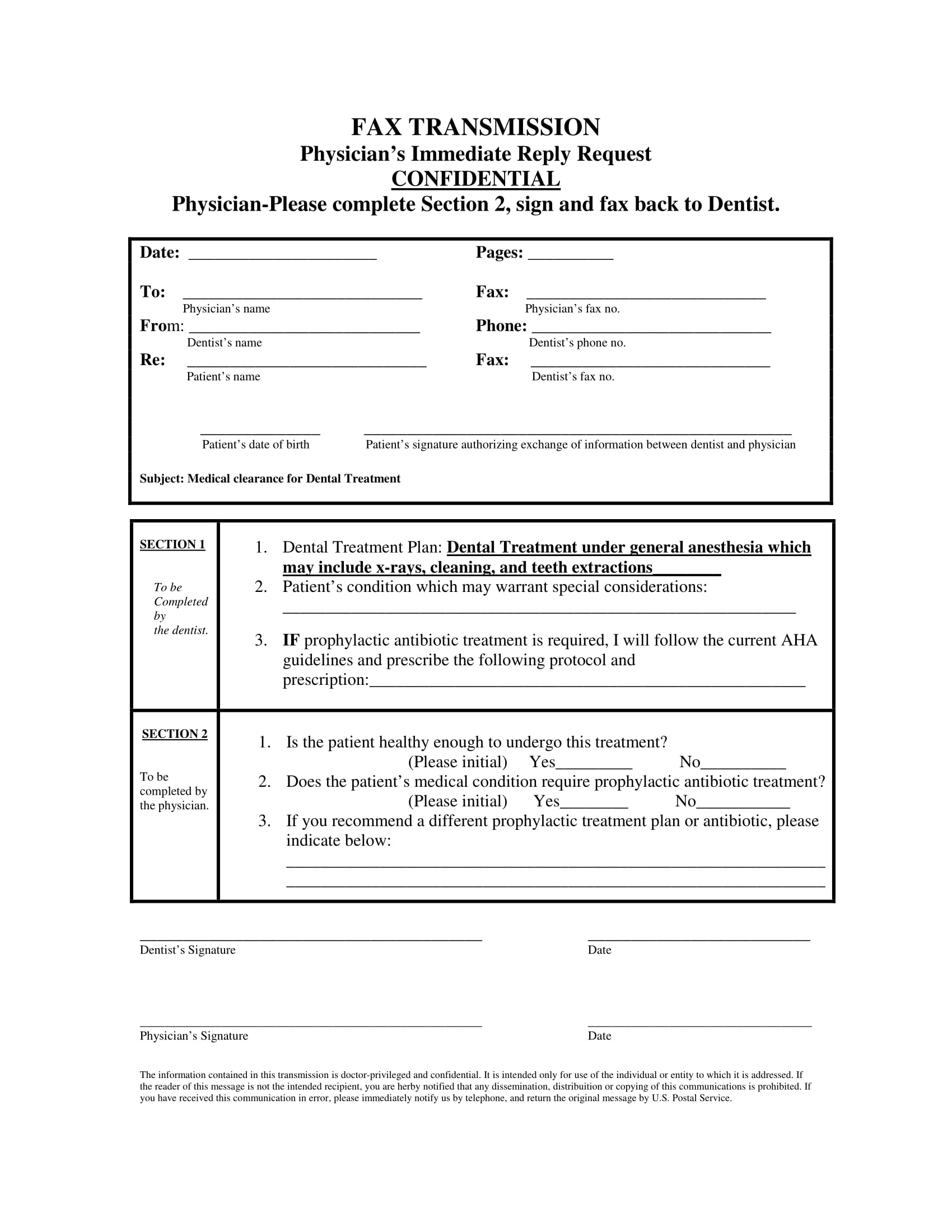
FREE 14+ Dental Medical Clearance Forms in PDF MS Word

Printable Dental Clearance Form Printable World Holiday
Printable Medical Clearance Form For Dental Treatment
FREE 14+ Dental Medical Clearance Forms in PDF MS Word

Dental Clearance Form Template 123 Form Builder
Printable Dental Clearance Form Printable Word Searches
Printable Dental Clearance Form For Surgery
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Printable Medical Clearance Form For Dental Treatment Printable Word
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Our Mutual Patient, As Noted Above, Is Scheduled For Dental Treatment At Our.
Web Find The Dental Clearance Letter You Want.
Edit Your Dental Clearance Form Pdf Online.
Easily Fill Out Pdf Blank, Edit, And Sign Them.
Related Post: