Printable Hipaa Release Form
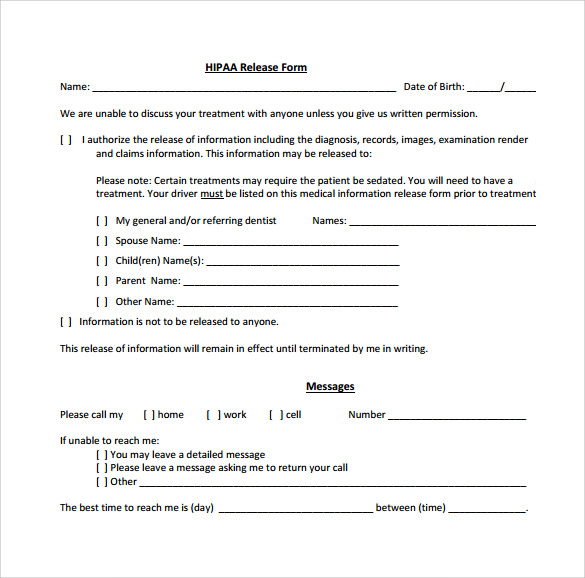
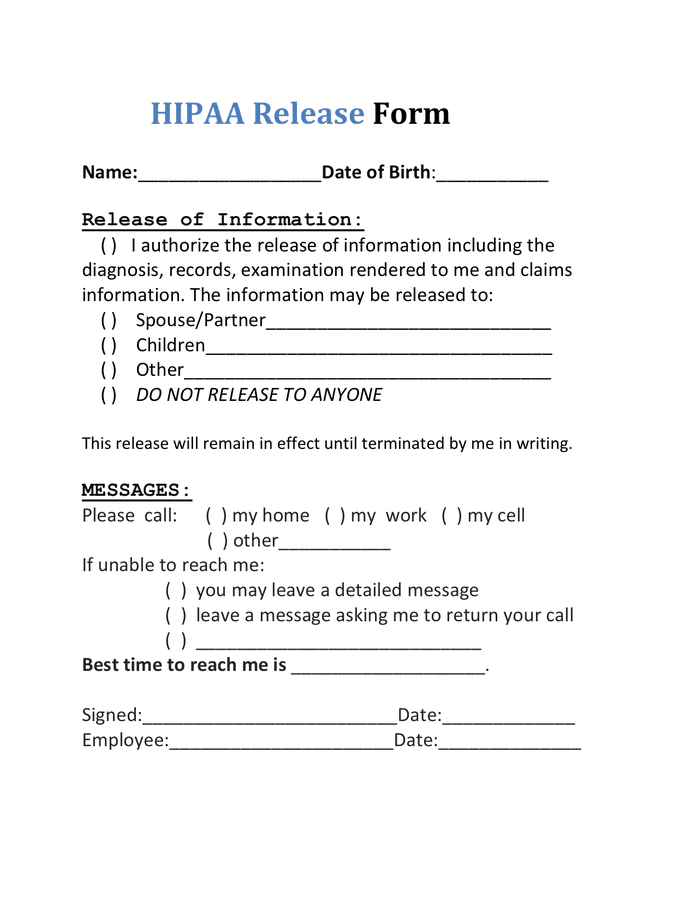
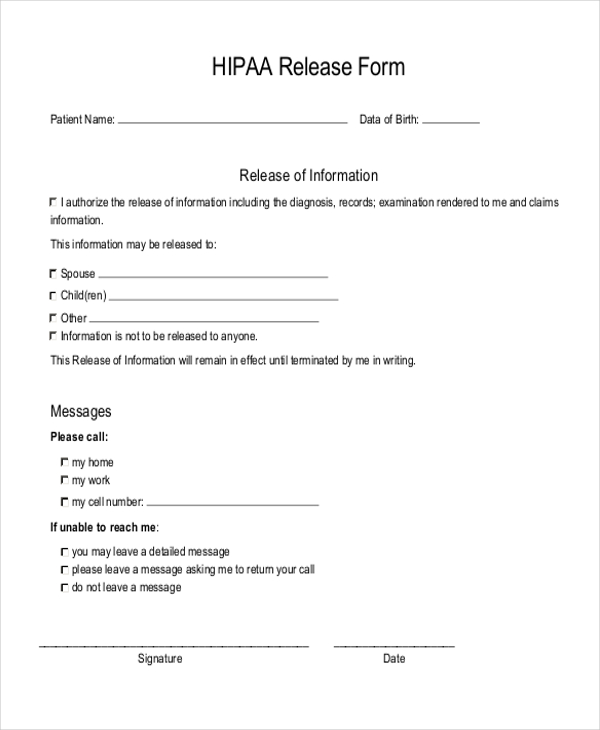
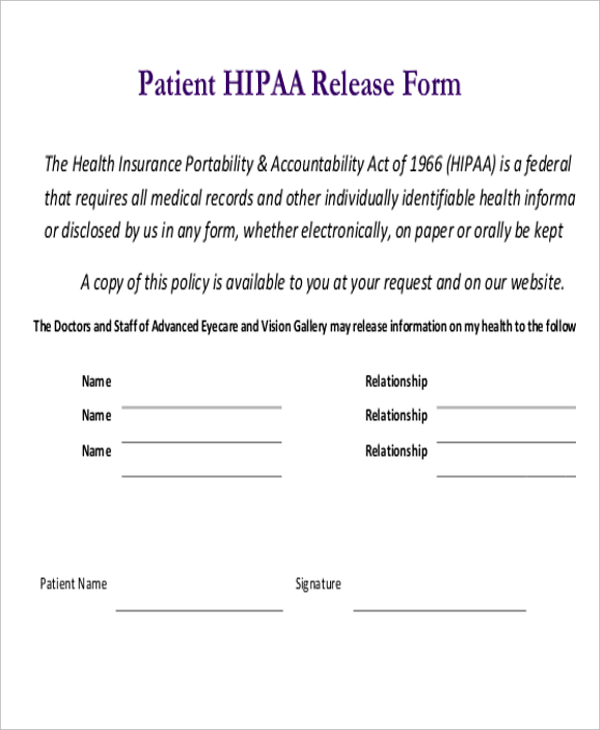
Printable Hipaa Release Form - Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. Free hipaa privacy authorization form template 3. Web updated august 10, 2023 hipaa forms are used in accordance with the health insurance portability and accountability act (hipaa) of 1996. Web the information requested on this form is solicited under title 38 u.s.c. Web as a reference, a release is known by other names: The form authorizes release of information in accordance with the health insurance portability and. Web hipaa release form please complete all sections of this hipaa release form. Templates built by legal professionals. Web this form may be used in place of doh2557 and has been approved by the nys office of mental health and nys office of alcoholism and substance abuse services to permit. At request of individual other: Date or event on which this authorization will expire: It also allows the added option for healthcare providers to share information. A medical release form can be revoked or reassigned at any time by the. Hipaa authorization for release of patient information form 4. This is the standard format of a hipaa release form and comprises of all the. As indicated on the form, specific authorization is required for the release of information about certain sensitive conditions,. Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. This form is to be used by a patient or legal representative to authorize the release. Web authorization for release of medical records to request release of medical information please complete and sign this form i,. If any sections are left blank, this form will be invalid and it will not be possible for your health. Tailored to fit your unique situation. Web what is the hipaa notice i receive from my doctor and health plan?. Save or instantly send your ready documents. Your health care provider and health plan must give you a notice that tells you how they may use and. Web the information requested on this form is solicited under title 38 u.s.c. Date or event on which this authorization will expire: The medical record information release (hipaa) form allows patients to give. Web what is the hipaa notice i receive from my doctor and health plan? Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. If not the patient, name of person signing form:. This form is to be used by a patient or legal. Web this hipaa release form pdf template is a standard release authorization form for disclosure of health information for healthcare and health insurance providers which the. Web hipaa disclosure authorization form. The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records. Developed by lawyers, customized by you. A medical. It also allows the added option for healthcare providers to share information. The form authorizes release of information in accordance with the health insurance portability and. Full name i hereby authorize to use or disclose my (discloser) protected health information related to (type of information) to for the. Web hipaa release form please complete all sections of this hipaa release. Hipaa authorization for release of patient information form 4. Your health care provider and health plan must give you a notice that tells you how they may use and. Web hipaa privacy authorization form **authorization for use or disclosure of protected health information (required by the health insurance portability and accountability act, 45. The form authorizes release of information in. At request of individual other: Authorization to disclose health information; Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. Web educational records that may contain health information. If not the patient, name of person signing form:. Web as a reference, a release is known by other names: Authorization to disclose health information; Ad download or email hipaa forms & more fillable forms, register and subscribe now! Web generic hipaa release form. Web 10.reason for release of information: Developed by lawyers, customized by you. The form authorizes release of information in accordance with the health insurance portability and. Easily fill out pdf blank, edit, and sign them. Web hipaa for individuals. Ad legally binding printable hipaa release form. It also allows the added option for healthcare providers to share information. If any sections are left blank, this form will be invalid and it will not be possible for your health. A medical release form can be revoked or reassigned at any time by the. Date or event on which this authorization will expire: This is the standard format of a hipaa release form and comprises of all the. Your health care provider and health plan must give you a notice that tells you how they may use and. Web hipaa disclosure authorization form. Web what is the hipaa notice i receive from my doctor and health plan? At request of individual other: Free printable hipaa release form template 2. Web generic hipaa release form. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. Tailored to fit your unique situation. Web 10.reason for release of information: Save or instantly send your ready documents. Web this hipaa release form pdf template is a standard release authorization form for disclosure of health information for healthcare and health insurance providers which the. Web the information requested on this form is solicited under title 38 u.s.c. Web what is the hipaa notice i receive from my doctor and health plan? Hipaa authorization for release of patient information form 4. Templates built by legal professionals. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. If not the patient, name of person signing form:. Date or event on which this authorization will expire: Full name i hereby authorize to use or disclose my (discloser) protected health information related to (type of information) to for the. This is the standard format of a hipaa release form and comprises of all the. At request of individual other: Save or instantly send your ready documents. If any sections are left blank, this form will be invalid and it will not be possible for your health. Tailored to fit your unique situation. Authorization to disclose health information; Web hipaa release form please complete all sections of this hipaa release form.
FREE 8+ Sample Hipaa Release Forms in PDF MS Word
FREE 9+ Sample Hipaa Forms in PDF MS Word
FREE 8+ Sample Hipaa Release Forms in PDF MS Word

FREE 10+ Medical Release Forms in PDF Excel MS Word
Printable Hipaa Forms Master of Documents
FREE 7+ Sample Hipaa Release Forms in PDF MS Word
HIPAA Release Form in Word and Pdf formats
FREE 11+ Sample HIPAA Release Forms in PDF MS Word
FREE 11+ Sample HIPAA Release Forms in PDF MS Word
FREE 8+ Sample Hipaa Release Forms in PDF MS Word
Web Generic Hipaa Release Form.
Web Hipaa For Individuals.
A Medical Release Form Can Be Revoked Or Reassigned At Any Time By The.
Learn Your Rights Under Hipaa, How Your Information May Be Used Or Shared, And How To File A Complaint If You Think Your Rights Were Violated.
Related Post: